What is new in adipose tissue?
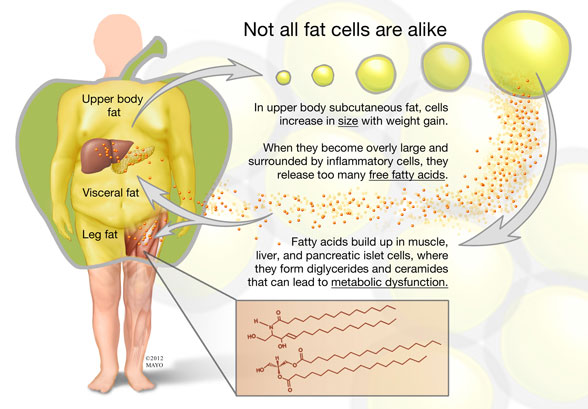
Men and women of normal weight have 15 percent and 30 percent body fat, respectively. Obese adults can have as much as 100 kg of body fat under extreme circumstances. The average size of a fat cell ranges from 0.2 to 1.4 mcg of lipid per cell, which means that someone with 20 kg of fat can have on the order of 33 billion fat cells. However, not all fat and not all fat cells are alike.
Michael D. Jensen, M.D., of the Division of Endocrinology, Diabetes, Metabolism, and Nutrition at Mayo Clinic in Rochester, Minn., says: "Our research program has focused largely on the attributes of human adipose tissue and body fat distribution as it relates to health and disease. For more than 20 years, we've been aware that persons with a preponderance of visceral (omental and mesenteric) fat and upper body fat are at greater risk for the metabolic complications of obesity. Persons with this body fat distribution also have greater concentrations of free fatty acid (FFA) in the blood."
Dr. Jensen continues: "It has been repeatedly shown that artificially elevating the FFA levels in healthy individuals can create insulin resistance and some of the other metabolic abnormalities seen in upper body obesity. One possible explanation is that those persons with excess visceral fat also take up and release too many fatty acids from the visceral fat. The adipocytes in the visceral fat, when studied in vitro, appear to have this potential. Excess FFA release from visceral fat could disproportionately affect hepatic metabolic function because the venous drainage of omental and mesenteric fat is into the portal vein — the so-called portal hypothesis.
"In contrast, adults with larger amounts of lower body (leg) fat often have relatively little visceral fat and have normal FFA levels. Our research has indicated that fat cells in visceral fat, leg fat and upper body subcutaneous fat have unique characteristics that make them almost completely different types of fat. We also have discovered that much of what was believed about the visceral fat in the portal hypothesis was not entirely correct."
Dr. Jensen explains: "For example, men and women with small visceral fat adipocytes have a much greater tendency to store fat in their visceral depot, probably because the levels of proteins and enzymes related to fat storage are quite high in these fat cells. However, as omental and mesenteric fat cells (and thus visceral fat mass) become larger, most of the proteins and enzymes related to fat storage are dramatically suppressed and the cells become resistant to fat storage.
"Under conditions of stable fat mass, one would predict that reduced fat storage would be accompanied by reduced FFA release. We have found that, consistent with this hypothesis, visceral fat is not a major source of fatty acids in the circulation of upper body obese or viscerally obese men and women. In fact, the high FFA levels found in upper body obesity come primarily from upper body subcutaneous fat. We also found that the liver is exposed to some extra FFAs coming from visceral fat in persons with large amounts of visceral fat. Leg fat and upper body subcutaneous fat also have their own unique characteristics that become even more apparent with weight gain."
Some adults develop new fat cells
When normal-weight people gain modest amounts of fat, they do so by enlarging the fat cells in their upper body subcutaneous fat depot. In contrast, gain of lower body fat is largely the result of increasing the number of fat cells. Dr. Jensen highlights: "We found that the gain of as little as 1.2 kg of leg fat resulted in an average gain of 2.6 billion new fat cells! This finding refuted the long-held belief that adult humans do not develop new fat cells but are instead stuck with those that developed in their adolescence. We recently reported that adults do not lose these new leg fat cells when they lose weight.
"New fat cells in adults, like new fat cells in children, come from preadipocytes. Preadipocytes are one of the most common cell types found mixed in among fat cells within adipose tissue. They are typically thought of as capable of replicating and, therefore, of generating a continuous potential supply of preadipocytes and adipocytes. When a preadipocyte receives an appropriate signal from the body, it will cease replicating and develop into a mature adipocyte, which then stores and releases fatty acids under relatively strict hormonal and neural control. Adipocytes also release various hormones, known as adipokines."
Dysfunctional release of fat cells
Dr. Jensen adds: "One of the recent hypotheses regarding why some people become metabolically ill when they become obese and others do not relates to dysfunctional storage and release of fatty acids by adipose tissue. When adipose tissue releases excessive amounts of fatty acids or cannot store them effectively, the fatty acids accumulate in so-called ectopic sites, such as visceral fat, muscle, liver, heart and islet cells. In these tissues, fatty acids can accumulate to excessive amounts in ceramides, diacylglycerols and long-chain acyl coenzyme A's. These fatty acid-containing molecules can serve a signaling function within cells and as such may cause insulin resistance and tissue dysfunction.
"Our laboratory is investigating why some tissues in some people convert fatty acids into abnormal amounts of signaling molecules and others are protected, either by not taking up fatty acids or by storing the fatty acids in the more benign triglyceride form. Understanding these pathways may provide an approach to preventing obesity-related metabolic disorders, such as insulin resistance diabetes, dyslipidemia and hypertension."
From Mayo Clinic Web Site
No comments:
Post a Comment